
As of the end of January national daily cases stand at about 150,000 down 40% from their peak of 250,000 early in the month. Still that’s more than twice the summer peak of about 70,000 The decline has been rapid, but seems to be moderating somewhat over the last week. Daily deaths, on the other hand, have been relatively stable at 3100 -3300 for the last 3 weeks. Here’s the graph since March.
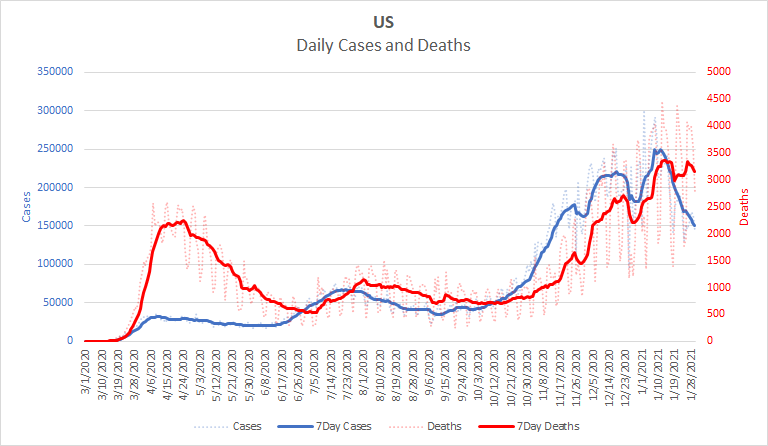
The easiest explanation for why deaths remain high is simply that deaths always lag infection. A 3 week lag is a bit longer that we have seen, but not alarmingly so. It’s also possible that we’re still seeing some effect of the holiday noise in the data. Deaths that may not have been fully reported in late December may be showing up in reports now. A third contributing factor may be improvements in treatment. We know that improved treatments have greatly reduced the fatality of COVID. Even in cases where patients end up dying, they may take longer to do so. I don’t have any data to support that; I haven’t seen any recent studies on the average duration of fatal cases. But it does seem reasonable that a treatment that is able to save one patient might merely delay death in a more severe case.
If you’re wondering whether the new variants could have anything to do with the high death rates, I think the answer is “no”. There is some evidence that the UK variant is more severe. However, the fact that we have only “some evidence” after this time means that it probably isn’t enough more severe to account for what we see in the graph. The South African variant does seem to be more severe but it is not yet widespread enough in the US to account for a noticeably higher death rate here.
The next week should bring some clarity on what’s behind the high death rates nationally. I expect we’ll see them come down. If we don’t, then look for some story or information that explains that.
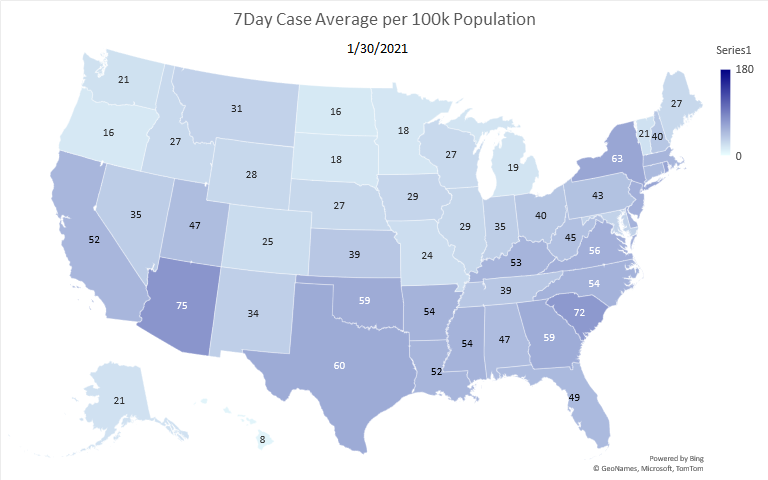
The decline in cases continues to be widespread. Only two states, Arizona and South Carolina are seeing more than 70 cases per 100,000 population now. 3 weeks ago, about half the states were that high. On the other hand, at the height of the summer surge, only one state was above 50. Here is the current map.
Here is the corresponding map for deaths.
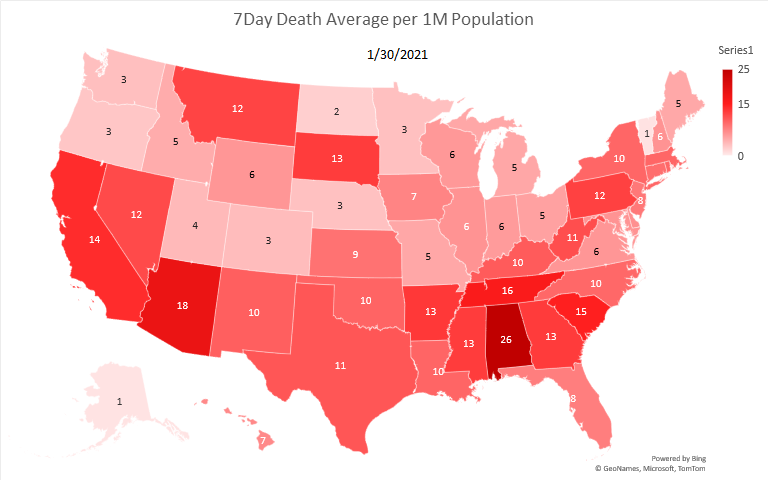
For the most part, the two maps mirror each other. The most notable exception is Alabama which has by far the highest death rate while being middle of the pack for cases. I don’t have a good explanation for this. It’s death rates have climbed for the last month while its case numbers have dropped. It may be worth keeping an eye on.
We’re definitely doing better with regard to cases. It’s tempting to breathe a small sigh of relief. But really, now is the time to double down on prevention. In the summer we worried that we might see as many as 100,000 cases per day. Now we’re seeing “only” 150,000. Don’t let the feeling of relief fool you. However much the situation has improved over the last few weeks, it is still quite dire.
Here’s a motivation for caution that you might not have thought of – it prevents dangerous variants. You’ve probably noticed that all of a sudden we have a lot of variants. Back in the summer it was just D614G. Now, there’s a UK variant, a South African variant and a Brazil variant. There’s even talk of a California variant. Why are there so many all at once? The answer is alarmingly simple, it’s because there are so many infections now. Mutations occur randomly when the virus reproduces. The more infections there are, the more the virus reproduces and the more mutations occur. The vast majority of mutations aren’t worth mentioning, but a few change the virus in important ways, making it more or less infectious and more or less severe. Some mutations can help it evade vaccinations. Indeed, one of the worries about the South Africa Strain is that the vaccines are not as effective against it. They still work, but not as well. Nobody can guess what the next variant will be like, but we do know that the more infections there are, the more variants we’ll see and the more likely we’ll see a dangerous one. The longer we stay at these high levels of infection, the more variants will evolve with the potential for ever more dangerous ones. We need to get our infection levels down to at least the summer levels, preferably lower, so that we aren’t generating new variants faster than we can respond to them.
This is why the idea that mask wearing and social distancing are “personal choices” is dead wrong. Every person who doesn’t abide by the restrictions endangers everybody else as they increase the risk not only of infecting others but of new dangerous variants. It’s sort of like saying that drunk driving is a personal choice. Yes, most drunk drivers manage to make it home OK most of the time. But every time anyone drives drunk, they increase the risk not only to themselves but to everyone around them. It’s a game of odds and society rightfully insists that we not endanger others by driving under the influence, no matter how inconvenient we find it to call a taxi or friend to come get us.
I also want to address one more issue that’s been getting some press. I’ve seen a number of articles lately warning that people who have been vaccinated can still spread the virus. We’ve seen multiple reports of people testing positive for COVID after having been vaccinated, e.g. Here’s why that happens.
First, no vaccines keep you from being infected with a virus. Vaccines never prevent viruses from infecting you, they just take care of the infections when they’re small enough to be harmless. Vaccines teach your immune system how to combat particular viruses. But your immune system only kicks in once it detects the virus and it takes a bit for it to ramp up the specific defenses. Typically, the immune system doesn’t reach full force until the virus has already invaded cells and started multiplying. At that point, the immune system can clear the virus and keep it from doing its usual harm. Vaccines prevent illness, not infection.
Now you may remember back to the spring when there was confusion about whether asymptomatic people could spread COVID. With most viruses, people aren’t infectious until they’re ill – until they have symptoms. So if a vaccine keeps you from being ill, it keeps you from being infectious. But COVID is different. COVID generates high viral loads very quickly, so you can transmit the virus to others before you become ill. The vaccines are very good at preventing people from becoming ill with COVID, but the virus ramps up quickly enough that it reaches transmission levels before our immune systems can clear it.
So, if you get vaccinated and breathe in some COVID virus, that virus very quickly starts reproducing in your upper respiratory tract and rapidly reaches detectable levels before your immune system is fully engaged. Since all that viral production is happening in your nose and throat, it’s very easy for you to shed virus as you breathe and talk even as your immune system is quietly and efficiently clearing the virus and keeping you from becoming ill. Of course the virus you shed may go on to infect someone who doesn’t have your resistance causing them to become gravely ill. This is why it’s important to continue with masks and social distancing even after getting vaccinated.
I encourage everyone to get vaccinated as soon as you possibly can. I certainly will. But once you’ve been vaccinated, it’s still your job to help protect others who haven’t been vaccinated. We owe each other this duty in the same way we owe all sorts of other duties, like not driving drunk.
So be safe and be well. We’ve got some more months to go before we can get past this pandemic. However, the safer we each are, the fewer months that will be.